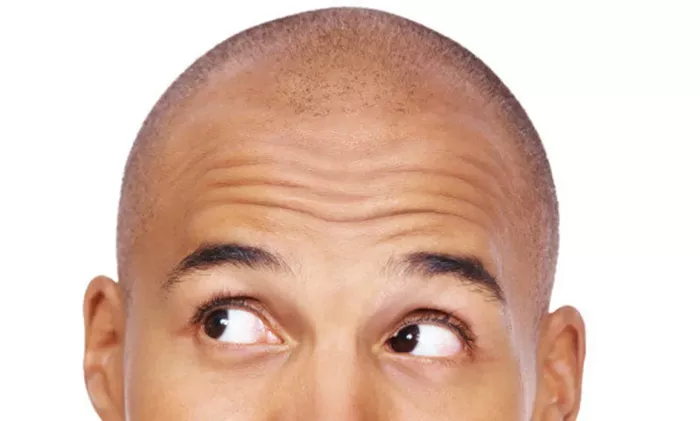
A 60-year-old man from West Java, Indonesia, was seen at the Department of Dermatology and Venereology, Hasan Sadikin General Hospital, Bandung, with thickened plaques and deep furrows on his forehead, creating a “leonine facies” appearance. These skin changes had first appeared 25 years earlier and had gradually increased in number, spreading to his neck and chest. The patient, a miner by profession, reported no other health problems and did not take regular medication. He was the third of nine siblings, with three of his brothers and sisters showing similar skin disorders starting around age 30. His twin brother had lesions identical to his own, while among his five children, two sons and one daughter had similar but milder symptoms. There was no family history of consanguineous marriage or significant medical issues.
On physical examination, the man showed thickened, coarse skin folds on his face, especially the forehead, producing a characteristic leonine facial appearance. A prominent protruding skin lesion measuring 3 cm long, 1 cm wide, and 1 cm thick was present on his left cheek. The affected facial skin felt greasy, but key areas around the eyes, nose, mouth, and ears were spared. His hair, nails, and teeth were normal, and there were no signs of acne or rosacea.
Biopsy samples from facial papules and nodules revealed multiple enlarged sebaceous glands in the dermis, consistent with sebaceous hyperplasia. Blood tests, serum biochemistry, chest X-rays, CT scans, and testosterone levels were all within normal limits.
The patient was diagnosed with familial presenile sebaceous hyperplasia (FPSH) associated with cutis verticis gyrata (CVG), a rare skin disorder marked by thickened, folded skin ridges mainly on the scalp and face. FPSH is a rare inherited form of sebaceous hyperplasia, which causes enlarged sebaceous glands and usually follows an autosomal dominant pattern with variable severity. The condition appeared in several family members, confirming a hereditary pattern.
Cutis verticis gyrata, first described in 1907, can be primary or secondary. Primary CVG often appears with neuropsychiatric conditions, while secondary CVG may develop due to systemic diseases or skin conditions such as sebaceous hyperplasia. The patient’s case is notable for the association of FPSH with CVG, both rare conditions that can involve systemic abnormalities.
Treatment options for CVG include surgical and conservative methods, with surgery being the most effective for managing severe skin folds. FPSH is a benign condition treated mainly for cosmetic reasons, with approaches such as electrosurgery, laser therapy, photodynamic therapy, and isotretinoin, though recurrences are common after treatment ends. Early diagnosis and multidisciplinary management are important to limit progression, especially in older patients.
This case highlights the challenges in diagnosing and managing rare skin conditions like FPSH combined with CVG and underlines the importance of thorough clinical and family evaluations.
Related Topics:























